
Fig. Various types of epicanthus
The epicanthus exists as a normal characteristic in Asian ethnicity, and it is peculiar to East Asians.
The epicanthus exists as a normal characteristic in Asian ethnicity, and it is peculiar to East Asians.
The epicanthus exists as a normal characteristic in Asian ethnicity, and it is peculiar to East Asians.
The epicanthus exists as a normal characteristic in Asian ethnicity, and it is peculiar to East Asians.
The true incidence of the Asian epicanthus is uncertain. But at least most people have the epicanthi of varying degree with absence or incomplete presence of supratarsal crease. Dr. Kwon reasoned that the epicanthus is a manifestation of the eyelid evolution by hypertrophy of the orbicularis oculi muscle. The affected areas of eyelid can be divided into three parts in aspect of their evolutional processes.
The manifestations of the eyelid evolution consists of 1) The epicanthus with vertical skin shortage and tension on upper medial eyelid, 2) The epiblepharon with loss of crease on the rest upper eyelid.
3) Skin fold on lower eyelid.
3) Skin fold on lower eyelid.

Examples) Typical Asian eye with a single eyelid accompanied with severe epicanthus
The epicanthus is a resultant manifestation by atrophy and fibrous degeneration of hypertrophied orbicularis oculi muscle after the active processes of the eyelid evolution. Von ammon first used the
term 'epicanthus' in 1860. For exact understanding about the evolution of eyelid, we need to define correctly the term “epicanthus” which means epicanthus itself with or without skin fold on lower eyelid equivocally. So far the epicanthus means“ a vertical fold of skin over the angle o fthe inner canthus”.
The expression word-‘fold’-is not good. And the commonly used term ‘epicanthal fold’ is inappropriate to describe the condition of Asian epicanthus. It may mislead plastic surgeons to understand epicanthus as
a fold. When we describe skin fold on lower eyelid-‘Epicanthus-related skin fold of lower eyelid’-is a more appropriate term considering its location.The epicanthus-related skin fold on lower eyelid is just skin fold by traction force which resulted from pulling-up of origin point during contraction of preseptal orbiculraris muscle. Formation of prominent fold on the lower eyelid is an ancillary manifestation which is formed between formation of epicanthus and complete loss of supratarsal crease over time.

Fig. (Left) A Caucasian eyelid on strong frowning who has hypertrophied orbicularis muscle., Notice angular point (point S) on which sheer stress is concentrated.
(Middle left) Asian single eyelid on strong frowning (Middle right) Relaxed eyelid with drawing of supratarsal crease. (Right) Open eyelid with crease formation by stick.
Von ammon first used the term 'epicanthus' in 1860. For exact understanding about the evolution of eyelid, we need to define correctly the term “epicanthus” which means epicanthus itself with or without skin fold on lower eyelid equivocally. So far the epicanthus means“a vertical fold of skin over the angle ofthe inner canthus”. The expression word-‘fold’-is not good. And the commonly used term ‘epicanthal fold’ is inappropriate to describe the condition of Asian epicanthus. It may mislead plastic surgeons to understand epicanthus as a fold.
When we describe skin fold on lower eyelid-‘Epicanthus-related skin fold of lower eyelid’-is a more appropriate term considering its location.The epicanthus-related skin fold on lower eyelid is just skin fold by traction force which resulted from pulling-up of origin point during contraction of preseptal orbiculraris muscle. Formation of prominent fold on the lower eyelid is an ancillary manifestation which is formed between formation of epicanthus and complete loss of supratarsal crease over time. Formation of epiblepharon is consequent to loss of mid-lateral crease and displacement of orbicularis muscle. The epiblepharon is a continuous structure with epicanthus in the upper eyelid and consists of the same composition as the epicanthus. The epicanthus and epiblepharon are purposeful structures of the evolutional process for eye protection, but the skin fold on lower eyelid is an unnecessary by-product. If we include the epicanthus itself and skin fold on lower eyelid into the meaning of ‘epicanthus’, the epiblepharon should be included also in the evolutional aspect.
It is appropriate that ‘epicanthus’ means epicanthus itself excluding skin fold on lower eyelid.
The main actor of eyelid evolution is the upper medial portion of preseptal orbicularis oculi muscle.The epicanthal skin region was originally crease. The epicanthus bulged from concave crease to convex shape with concurrent loss of medial crease consequent to detachment of aponeurotic expansion.
The shape of bulging convexity is due to gravitational displacement of anterior lamella including hypertrophied preseptal orbicularis muscle. So it would be reasonable that we call the epicanthus as ‘epicanthal bulging’ instead of 'epicanthal fold.’ Nevertheless, bulging or fold only means or indicates a part of affected eyelid areas. So we think that we need to better define each part ‘epicanthus’, ‘epiblepharon’,'epicanthus-related skin fold’ separately to remove any confusion.

Examples) Combined magic epicanthoplasty and non-incisional double eyelid surgery
The epicanthus exists as a remnant fibromuscular volume on the upper medial canthal region with vertical(actually diagonal, relative meaning in relation to horizontal supratarsal crease) skin shortage and tension which causes difficulty in horizontal skin folding. It acts as a major hindrance of a double eyelid formation in Asian blepharoplasty. The fibrous tissues and malpositioned orbicularis muscle prevents the even transmission of levator muscle power toward the medial skin because the aponeurotic fibers have been detached and do not extend to the epicanthal skin area any more.
The preexisting vertical skin tension acts as tensional stress on newly formed surgical crease.
The epicanthus The epicanthal skin tension is considered as a major factor which inhibits the sustainability of surgical crease in Asian double eyelidplasty. Also, the malpositioned orbicularis muscle can be reactivated as a vertically acting inhibitor which causes active tensional stress on mid-lateral surgical crease, especially when we have performed the outfold type double eyelidplasty without epicanthoplasty.
The epicanthus The epicanthus veils various amounts of inner medial canthus, so it makes Asian eyes look stuffy aesthetically.
The preexisting vertical skin tension acts as tensional stress on newly formed surgical crease.
The epicanthus The epicanthal skin tension is considered as a major factor which inhibits the sustainability of surgical crease in Asian double eyelidplasty. Also, the malpositioned orbicularis muscle can be reactivated as a vertically acting inhibitor which causes active tensional stress on mid-lateral surgical crease, especially when we have performed the outfold type double eyelidplasty without epicanthoplasty.
The epicanthus The epicanthus veils various amounts of inner medial canthus, so it makes Asian eyes look stuffy aesthetically.
Evolution of the Epicanthus (Kwon’s Theory)

Fig. The evolutionary process of the eyelid
Underdeveloped nasal bone, excess of horizontal medial canthal skin relative to the vertical skin shortening, excess of orbicularis muscle and abnormal skin tension are described as causes of the epicanthusby plastic surgeons previously.
There is an anthropological hypothesis that the epicanthus is an outward phenotype which is the result
of evolution for adaptation to relevant environments. Genetically, all modern humans are included into the subspecies Homo sapiens sapiens,i.e. the subspecies ofHomo sapiens. It has been reasoned that the racial differences of modern humans are just phenotypic variations. But, the developmental mechanism of Asian epicanthus was not suggested clearly.
Dr. Kwon reconsidered basically without stereotype for the epicanthus. As is the standard for all evolutionary adaptations, the human muscle system would evolve in its efforts to increase survivability. It is clear that the evolution of eyelid muscles are based upon how humans operated in the relevant environments.
Anthropologists had already presumed the strong UV, Siberian cold, yellow dust of northeast of Asia as causes of the epicanthus. There would be strong repeated contraction of upper orbicularis muscle and depressor supercilli muscle in Asian eyelid for frowning. Excessive muscle contraction would be inevitable action for protection of eyes from environmental harshness. Environmental adaptation would be a basic cause for formation of the epicanthus.
Dr. Kwon suggested Kwon's theory for the evolution of Asian eyelid
Underdeveloped nasal bone, excess of horizontal medial canthal skin relative to the vertical skin shortening, excess of orbicularis muscle and abnormal skin tension are described as causes of the epicanthusby plastic surgeons previously.
There is an anthropological hypothesis that the epicanthus is an outward phenotype which is the result
of evolution for adaptation to relevant environments. Genetically, all modern humans are included into the subspecies Homo sapiens sapiens,i.e. the subspecies ofHomo sapiens. It has been reasoned that the racial differences of modern humans are just phenotypic variations. But, the developmental mechanism of Asian epicanthus was not suggested clearly.
Dr. Kwon reconsidered basically without stereotype for the epicanthus. As is the standard for all evolutionary adaptations, the human muscle system would evolve in its efforts to increase survivability. It is clear that the evolution of eyelid muscles are based upon how humans operated in the relevant environments.
Anthropologists had already presumed the strong UV, Siberian cold, yellow dust of northeast of Asia as causes of the epicanthus. There would be strong repeated contraction of upper orbicularis muscle and depressor supercilli muscle in Asian eyelid for frowning. Excessive muscle contraction would be inevitable action for protection of eyes from environmental harshness. Environmental adaptation would be a basic cause for formation of the epicanthus.
Dr. Kwon suggested Kwon's theory for the evolution of Asian eyelid

Fig. The stage of the eyelid evolution according to the main action of orbicularis oculi muscle in Kwon’s theory. Loss of medial crease, formation of the epicanthus, loss of mid-lateral crease, formation of the epiblepharon occur in sequence. I. Stage of hypertrophy: The hypertrophy of orbicularis oculi muscle and depressor supercilli muscle develop by repeated frowning. The hypertrophy of orbicularis oculi muscle cause attenuation of the aponeurotic expansion which penetrate through orbicularis muscle. The aponeurotic penetrations
loosen and become sparse.
II. Stage of sheer stress: Complete detachment of aponeurotic expansions with loss of supratarsal crease takes place on point S by sheer stress. The detachment of aponeurotic fibers can occur beneath the orbicularis muscle or on the orbicularis muscle. Orbicularis oculi muscle contraction acts as sheer tensional stress with depressor supercilli muscle. The depressor supercilli muscle plays an ancillary role.
III. Stage of tensional stress: The successive loss of medial crease below point S results from displacement of preseptal orbicularis oculi muscle toward eyelash and the vicious cycle between malpositioned muscle hypertrophy and crease loss. The orbicularis oculi muscle contraction mainly act as tensional stress on remaining aponeurotic fibers and medial crease.
IV. Stage of compressional stress: Excessive contraction of orbicularis oculi muscle acts as compressional stress on overlying skin of upper medial eyelid with resultant vertical skin shortage and tension. The tight tension band develops due to vertical skin shortening of upper medial eyelid.
V. Stage of traction and tensional stress: Contraction of orbicularis oculi muscle acts as tensional stress on remaining supratarsal crease resulting in successive loss of supratarsal crease on the upper eyelid superiorly and/or act as traction force causing skin tent toward point P on the lower eyelid inferiorly. During and after formation of a tight tension band by vertical skin shortage, the orbicularis oculi muscle contraction causes a prominent skin fold on the lower eyelid by pulling-up the muscle point of origin like setting up a tent pole during contraction. The preseptal orbicularis muscle pulled up its origin superolaterally with skin tent on lower eyelid during contraction.
VI. Stage of degeneration: The atrophy of orbicularis oculi muscle and accompanying degenerative fibrosis develop, leaving the epicanthus with incomplete crease or epicanthus without crease.
The hypertrophied orbicularis oculi muscle becomes atrophied and replaced by fibrosis, but there remains vertical skin shortage and tension left on upper eyelid and skin fold and wrinkles on lower eyelid. Also there has been left centripetal fibrosis toward point p under the skin of lower eyelid.
loosen and become sparse.
II. Stage of sheer stress: Complete detachment of aponeurotic expansions with loss of supratarsal crease takes place on point S by sheer stress. The detachment of aponeurotic fibers can occur beneath the orbicularis muscle or on the orbicularis muscle. Orbicularis oculi muscle contraction acts as sheer tensional stress with depressor supercilli muscle. The depressor supercilli muscle plays an ancillary role.
III. Stage of tensional stress: The successive loss of medial crease below point S results from displacement of preseptal orbicularis oculi muscle toward eyelash and the vicious cycle between malpositioned muscle hypertrophy and crease loss. The orbicularis oculi muscle contraction mainly act as tensional stress on remaining aponeurotic fibers and medial crease.
IV. Stage of compressional stress: Excessive contraction of orbicularis oculi muscle acts as compressional stress on overlying skin of upper medial eyelid with resultant vertical skin shortage and tension. The tight tension band develops due to vertical skin shortening of upper medial eyelid.
V. Stage of traction and tensional stress: Contraction of orbicularis oculi muscle acts as tensional stress on remaining supratarsal crease resulting in successive loss of supratarsal crease on the upper eyelid superiorly and/or act as traction force causing skin tent toward point P on the lower eyelid inferiorly. During and after formation of a tight tension band by vertical skin shortage, the orbicularis oculi muscle contraction causes a prominent skin fold on the lower eyelid by pulling-up the muscle point of origin like setting up a tent pole during contraction. The preseptal orbicularis muscle pulled up its origin superolaterally with skin tent on lower eyelid during contraction.
VI. Stage of degeneration: The atrophy of orbicularis oculi muscle and accompanying degenerative fibrosis develop, leaving the epicanthus with incomplete crease or epicanthus without crease.
The hypertrophied orbicularis oculi muscle becomes atrophied and replaced by fibrosis, but there remains vertical skin shortage and tension left on upper eyelid and skin fold and wrinkles on lower eyelid. Also there has been left centripetal fibrosis toward point p under the skin of lower eyelid.
Kwon’s Classification of the epicanthus in relation to supratarsal crease.

Fig. Classification of the epicanthus in relation to supratarsal crease.
Type I : Attenuated original crease without epicanthus (exopthalmic Asian eyelid)
Type II : Minimal epicanthus without crease. (without epibepharon)
Type III : Epicanthus with attenuated original crease
Type IV : Epicanthus with lowered infold crease
Type V : Epicanthus without crease (epicanthus and epiblepharon).
The epicanthus is a remnant manifestation of eyelid evolution which resulted from hypertrophy of upper orbicularis muscle and related aponeurotic attenuation. . Increased blood supply induced by hypertrophied orbicularis muscle and climate factors would cause hypertrophy and pseudoherniation of preaponeurotic fat. Displacement of orbicularis muscle and fat pad would affect the levator muscle and Muller’s muscle.
A relatively longer medial canthal ligament and underdeveloped nasal bone would be additional evolutional manifestations by hypertrophy of the orbicularis oculi and excessive tension. Under this theory, the main purposes of Asian epicanthoplasty would be the anatomical restoration of medial canthus and eyelid soft tissues which are basicfor double eyelid formation in Asian eyelids.We could apply the devolutional concept which reverses evolutionary processes in Asian epicanthoplasty.

Example) Magic epicanthoplasty combined with a non- incisional double eyelid surgery

Example) Magic epicanthoplasty combined with a incisional double eyelid surgery

Example) Magic epicanthoplasty combined with a incisional double eyelid surgery
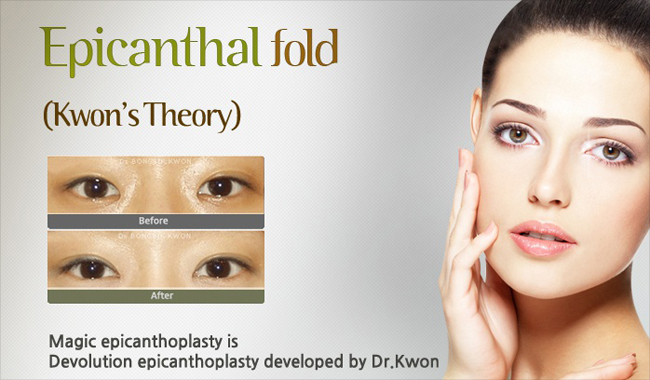
What is epicanthoplasty (correction of epicanthal folds)?
Epicanthoplasty is the name of the surgery that corrects epicanthal folds that cover the inner corner of Asian eyes, so that your eyes look more open and become more refined and bigger. For those who have a wide distance between eyes or has small eyes, or looks severe because of inclination of the inner corner of your eyes by a epicanthal fold, the epicanthoplasty is helpful. When it is performed with a double eyelid surgery at the same time, the horizontal length of eyes can be extended and the interepicanthal distance will also be narrowed effectively. Also, attractive and refined double eyelids will be created by improvement of the epicanthal folds.
Double eyelidplasty is the most frequent cosmetic procedure for Asians, and the epicanthus was a conundrum which limit cosmetic result of double eyelidplasty. Double eyelidplasty without epicanthoplasty tend to be unattractive or unnatural. Aesthetically, the epicanthal fold is worsened when performing double eyelidplasty without epicanthoplasty, because double eyelid formation aggravates vertical tension on epicanthal skin. It has been a long-standing dilemma for plastic surgeons which procedure to choose, i.e. infold type double eyelidplasty with a less satisfactory result or outfold type double eyelidplasty with concomitant epicanthoplasty, taking risk of hypertrophic scar in Asian eyelid. When the epicanthal fold is severe, the surgical incision of skin flap also become longer, and a scar could be easily visible in conventional method, which based on the concept of local skin flap and lacked a consideration of upper orbicularis muscle and vertical epicanthal tension.
Although it has been reasoned that combined epicanthoplasty is helpful in Asian double eyelidplasty, there has not been clear understanding about epicanthal fold, resulting in controversies for solution. There have been so many epicanthoplasty methods developed in its early days, which are mostly based on skin flap concept. Currently using methods are combined technics including skin excision, z-plasty, myotomy or myectomy of preseptal orbicularis muscle, skin redraping, plication of medial canthal ligament and so on. The development of incomplete methods were unavoidable without understanding about true nature of the epicanthus. As the clinical significance of the epicanthus is mainly related with Asian double eyelidplasty, essential epicanthoplasty should be a key to plastic surgeons for choice of all the type of double eyelid including high outfold type(parallel type). But, there has not yet been a potent epicanthoplasty method which deserves universal solution for Asian double eyelidplasty. So we developed Kwon's method based on devolutional concept.
Double eyelidplasty is the most frequent cosmetic procedure for Asians, and the epicanthus was a conundrum which limit cosmetic result of double eyelidplasty. Double eyelidplasty without epicanthoplasty tend to be unattractive or unnatural. Aesthetically, the epicanthal fold is worsened when performing double eyelidplasty without epicanthoplasty, because double eyelid formation aggravates vertical tension on epicanthal skin. It has been a long-standing dilemma for plastic surgeons which procedure to choose, i.e. infold type double eyelidplasty with a less satisfactory result or outfold type double eyelidplasty with concomitant epicanthoplasty, taking risk of hypertrophic scar in Asian eyelid. When the epicanthal fold is severe, the surgical incision of skin flap also become longer, and a scar could be easily visible in conventional method, which based on the concept of local skin flap and lacked a consideration of upper orbicularis muscle and vertical epicanthal tension.
Although it has been reasoned that combined epicanthoplasty is helpful in Asian double eyelidplasty, there has not been clear understanding about epicanthal fold, resulting in controversies for solution. There have been so many epicanthoplasty methods developed in its early days, which are mostly based on skin flap concept. Currently using methods are combined technics including skin excision, z-plasty, myotomy or myectomy of preseptal orbicularis muscle, skin redraping, plication of medial canthal ligament and so on. The development of incomplete methods were unavoidable without understanding about true nature of the epicanthus. As the clinical significance of the epicanthus is mainly related with Asian double eyelidplasty, essential epicanthoplasty should be a key to plastic surgeons for choice of all the type of double eyelid including high outfold type(parallel type). But, there has not yet been a potent epicanthoplasty method which deserves universal solution for Asian double eyelidplasty. So we developed Kwon's method based on devolutional concept.
<Teuim Clinic Dr.Kwon>
E-mail : paris85@naver.com